The quality of a life may be seen as a balance between wellbeing, and suffering. This view provides us with two targets if we seek to utilise our resources to improve lives, namely:
To prevent or reduce suffering (alleviation)
To promote or enable wellbeing (facilitation)
The first removes the barriers individuals face in pursuit of a life of wellbeing. Ill-health, lack of education, inadequate economic resources all limit an individual’s ability to pursue their goals and fulfil their desires. It seeks to free the individual from external constraints which inhibit their ability to express autonomy and satisfy their preferences.
This is in opposition to the second aim. The second aim works to facilitate the satisfaction of desires. Social pursuits, the arts and leisure activities are all in addition to the basic needs required for an autonomous existence, allowing for an individual to be free to pursue the satisfaction of their preferences.
The alleviation approach is generalisable to all people regardless of preferences, desires, politics, age or gender. Improving ill-health, lack of education or economic hardship at scale is likely to positively impact a large proportion of a society. On the contrary, the facilitation approach requires nuance and an understanding of goals and preferences of the individual. It would not be easy on a global scale to suggest an intervention or policy that would enable the preference satisfaction of all, or even most, of humanity, unless it were the provision of some generic instrumental resource such as money. Facilitation needs to be more tailored to those it seeks to serve. In a religious society for instance, a place of worship may provide significant benefit in terms of preference satisfaction for its people, whilst implementation of the same project in a religiously agnostic society would have a neutral, or potentially negative, impact.
Given the constrained resources available to individuals and communities, consideration needs to be given to the relative ‘good’ that is achieved via each approach. By treating a chronic health condition that subtracts from the wellbeing of an individual, are we doing more for that individual than a service that, at a similar scale, facilitates the same individual pursuing their favoured leisure activities? One view on this issue may posit that the alleviation approach better enables the individual to engage, enjoy and find fulfilment in every aspect of their being. It is further likely that an asymmetry exists between equal absolute amounts of alleviation and facilitation, given the human tendency toward loss aversion.
I would now like to consider the utilitarian approach to this calculus, and draw on virtue ethics in an attempt to explore this issue more broadly. But first a quick digression on Maslow’s hierarchy of needs, as I think this is highly relevant when considering these issues.
Maslow’s Hierarchy
It may feel intuitive that more base requirements (such as safety, health, adequate nutrition) need to be met, before considerations of esteem, or self realisation can be materialised. If we accept this view, there is a strong case to be made that the alleviation approach is a necessary precondition to the facilitation approach. However a strict ranking in the sense of a hierarchy of needs seems to deprive those who’re yet to satisfy the base requirements of the experiences found toward the top of the hierarchy. A strong argument could be made that despite hunger or a lack of safety, one may hold self-esteem or hopes for self-realisation as important goals, which they would be happy to satisfy despite otherwise lacking the resources to satisfy every need below on the hierarchy. Thinking of wellbeing in this linear, or hierarchical, format tends to miss something important about what constitutes a life well lived for any one individual.
Utilitarianism
If we assume a basic form of utilitarianism, that is of a continuum from negative to positive utility, we can more easily frame the two approaches of alleviation and facilitation. One may see the alleviation of suffering as movement from a state of very low (or negative) utility upward along the gradient, and the enabling of wellbeing as a further move upward toward more positive utility. The simplicity of such a conception is tempting. The framing may be somewhat complicated if we consider where the point of neutral utility lies. Does positive movement on the left of the neutral point hold different weight to a corresponding movement on the right of the neutral point? Should the continuum be considered as a linear relationship between resources invested and utility improved?
This formulation of utilitarianism may hold that there is not a qualitative difference between the alleviation and facilitation approaches. The simplicity of this framing and potential comparability amongst its practical implications are a large draw card, however it does risk missing the fact a qualitative distinction may be necessary, and important, in questioning whether an alleviation or a facilitating approach is what is best to do. In consideration of what it truly means to live a flourishing or satisfactory human life, it is not the mere absence of negative experience.
Virtue Ethics
Virtue ethics posits that human life is in pursuit of a state of eudaimonia, a state of wellbeing and human flourishing through the enactment of virtuous acts. Acting in accordance with the virtues, such as justice, courage, wisdom, moves one toward a state of eudaimonia. What constitutes an act in accordance with the virtues is highly subjective and context dependent. An individual may lead a virtuous life in pursuit of eudaimonia with any level of resource. The Virtue ethics approach does not fit onto a linear scale in the same way a simplified formulation of utilitarianism might, but I feel may more closely approximate what it is any one individual seeks to optimise for.
Alleviation under this model would hold similar benefits as previously outlined, in that it could be seen as good irrespective of the individual’s pursuit of virtue and eudaimonia. Facilitation again may present difficulties, as attempting to scale up an individual’s sense of justice, courage or wisdom may be challenging, given their highly contextual natures. Considering the problem through the lens of virtue ethics I believe allows for a more realistic appreciation of the complexities inherent in the facilitation approach.
Conclusion
A non-controversial claim is that anyone with altruistic motives seeks to give others what they themselves would consider a meaningful life. Tension exists about what it means to live a meaningful life. A meaningful life does not come alone from the absence of disease, infirmity, economic hardship or lack of education. Meaning can be sought amongst poverty and disease, and those with plentiful resources can long for meaning. However, the alleviation approach, in contrast to the facilitation approach, offers a more broadly good means of doing good. It is not as sensitive to individual preferences, and offers a platform from which individuals can pursue actualisation or the attainment of flourishing. As such, it is likely a more effective means of doing good.
Hepatitis B is a highly prevalent and consequential viral infection. Hepatitis B was responsible for approximately 18.2 million DALYs in 2019. It has a global prevalence of ~4%.
Globally, rates are improving. The African region has an under 5 prevalence rate of 2.7% and is a potential geographical focus area to scale up preventative efforts.
Approximately 35-50% of cases of chronic Hep B are acquired as a result of mother to child transmission during delivery.
A rapid diagnostic test is available for HBV. A cheap and effective vaccination is available to prevent mother-to-child transmission. Anti-viral medication are effective in avoiding complications of chronic infection and preventing mother-to-child transmission.
Vaccination, especially birth dose vaccination, is under utilised, especially in the African region.
Scaling up interventions to prevent mother-to-child transmission, such as birth dose vaccination or peripartium antiviral prophylaxis, in high prevalence regions could be particularly cost-effective, especially if layered on or implemented alongside other maternal health interventions.
Key Uncertainties
Studies of global prevalence, complications and DALYs associated with hepatitis B are based off modelling, and there may be greater uncertainty around figures in areas where healthcare data is lower quality.
The Cochrane review on interventions to prevent mother-to-child transmission may have overrepresented infants born to HBeAg positive mothers (as e antigen status was not reported in a number of the included studies), these results need to be interpreted with caution.
There is little data available on the impact of HBV birth dose vaccine alone, independent of the 3 dose vaccine schedule recommended by WHO.
A note on terminology
Hepatitis B is associated with confusing terminology.
HBsAg refers to hepatitis B surface antigen, refers to current hepatitis B infection.
HBeAg refers to hepatitis B e antigen, refers to current infection, active viral replication and a high infectivity state.
HBV DNA is a quantitative measure of virus in the blood.
What is Hepatitis B?
Hepatitis B is a disease caused by the Hepatitis B Virus (HBV). It can cause both an acute, and chronic hepatitis (liver infection). It is transmitted via body fluids (blood, saliva, semen or vaginal fluid) from an individual with an active viraemia (HBV circulating in the blood). Transmission can occur horizontally (from person to person) or vertically (from mother to child). Neonates and infants are most susceptible to progress to chronic infection when exposed to HBV, this most commonly occurs during delivery to a mother with active hepatitis B. Acute hepatitis B rarely requires specific treatment and is cleared in that majority of immunocompetent adults. Chronic hepatitis B (CHB) risks progressing to cirrhosis (liver scarring and failure), and CHB related liver cancers, which account for the majority of the burden of disease associated with hepatitis B. Hepatitis B is a vaccine preventable illness, delivered as a 3-4 dose regimen with a ‘birth-dose’ given to a neonate soon after delivery. Treatment in the form of anti-viral medications are available to suppress viral replication in those with established CHB, this prevents complications but rarely cures the disease.
Approximately 316 million people were infected chronically with HBV in 2019. There were approximately 331 000 deaths from HBV related cirrhosis, and 192 000 deaths from HBV related liver cancer.1 Hepatitis B resulted in approximately 18.2 million DALYs in 2019.2 The World Health Organisation in 2022 set a goal of elimination of AIDS, viral hepatitis and sexually transmitted infections by 2030. WHO has additionally focussed on a ‘triple-elimination’ initiative, focussing on the elimination of mother-to-child transmission (MTCT) of syphilis, HIV and HBV, given their shared modes of transmission and epidemiological risk factors.
Importance
What is the natural history of Hepatitis B?
Infection with HBV is virologically and immunologically complex. Infection can be conceptually delineated by a range of serological, virological and biochemical factors into phases of illness. Individuals exposed to HBV may develop an acute phase of the illness, related to viral replication in the host’s hepatocytes (liver cells). Clinically this may manifest as an acute hepatitis (presenting with liver pain, fever and jaundice), or may cause a mild non-specific illness. Acute illness is typically self-limiting with only supportive treatment required. There is a ~1% risk of acute illness progressing to acute liver failure.3 Acute liver failure has a mortality of 65-85%.4
CHB is defined as serological positivity >6 months after disease onset. Chronic infection causes morbidity and mortality by two main mechanisms, increasing the risk of cirrhosis, and HBV related liver cancers. Approximately 15-40% of those with untreated CHB will progress to cirrhosis or liver cancer.5 Development of cirrhosis and liver cancer is a result of prolonged viral replication and an associated inflammatory response. Cirrhosis and liver cancer take approximately 10-20 years to develop.4 Treatment with anti-viral medication and viral suppression reduces the risk of complication from chronic infection significantly.
Not all individuals exposed to HBV will go on to develop CHB. The risk of progressing to CHB after exposure is inversely related to age at time of first exposure.6 Neonates have an 40-90% risk of progression if born to a Hep B positive mother (can be >95% if mother is HBeAg positive), children <6 have an approximate 30% risk, and healthy adults have a risk of approximately <5%.7 It is postulated that approximately 35-50% of all CHB cases worldwide are due to mother to child transmission.8
The exact mechanism of vertical transmission is not entirely clear. Intrapartum or peripartum (during or around the time of delivery) is thought to be the predominant mechanism by which HBV is transmitted from mother to child. There may be a smaller role on intrauterine transmission (during pregnancy, prior to delivery). There is insignificant evidence to suggest transmission via breast milk.4
Hepatitis B requires serology for diagnosis. There are a range of serological markers tested for which can help clinicians differentiate current infection, past or cleared infection, vaccination, or susceptibility if exposed. If chronic infection is suspected further investigation including viral load and genotyping can be performed, as well as investigation for complication of disease. Rapid diagnostic testing (RDT) is emerging as an easy to interpret, cheap and quick alternative to serological testing in resource constrained settings. Specificity for RDTs is 98.3 to 99.3%, and sensitivity is >99% for HBsAg.9 Whilst only providing information on HBsAg status (presence or absence of HBV in the blood), they offer an accessible alternative to formal serology in resource constrained settings.
What is the burden of Hepatitis B worldwide?
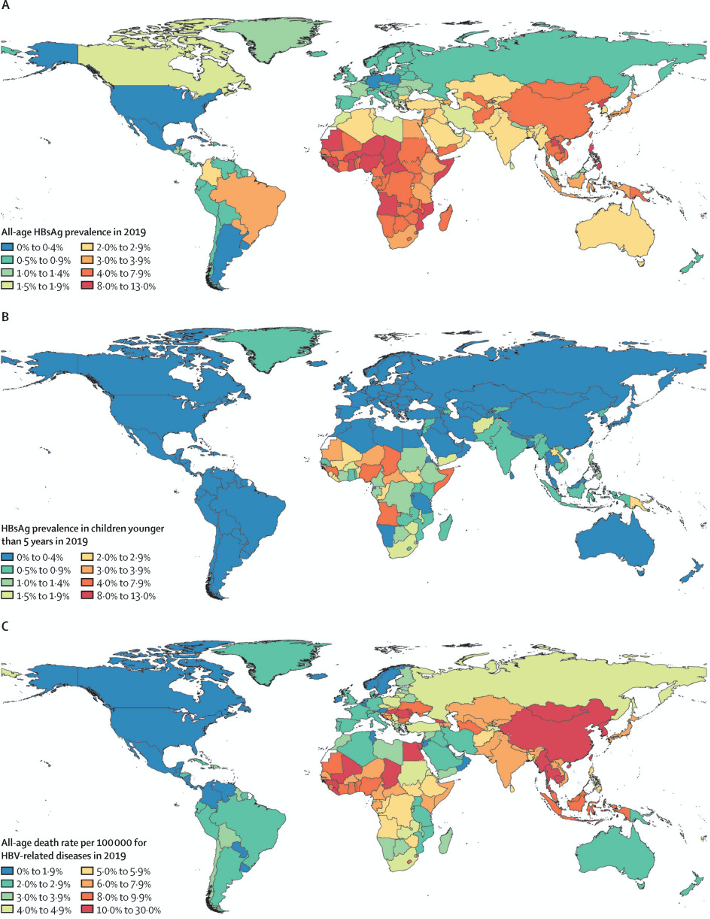
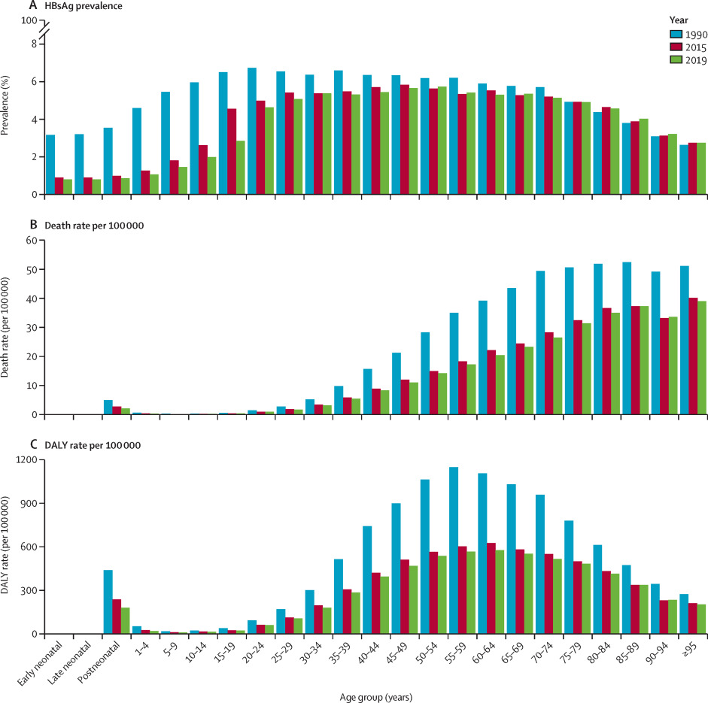
Based on available seroprevalence data, it is estimated that 4.1% (95% uncertainty interval (UI) 3.7-4.5%) of the global population had chronic Hep B infection in 2019. The rate varied widely across regions. The WHO Western Pacific region had a prevalence of 7.1% (95% UI 6.3 to 7.9), the African region had a prevalence of 6.5% (5.8 to 7.3). The European region had a prevalence of 1.1% (95% UI 1.0 to 1.2). Seroprevalence of children under 5 globally was 1.0% (95% UI 0.8 to 1.2). All WHO regions had an under 5 seroprevalence of <1%, except the African region at 2.7% (95%UI 2.2 to 3.2).6
HBV was responsible for approximately 18.2 million DALYs in 2019.2 Of these, 70% were attributable to 10 countries (in order: China, India, Indonesia, Nigeria, Pakistan, Egypt, Thailand, South Korea, Bangladesh, Myanmar). HBV related disease (acute hepatitis, cirrhosis and liver cancer related to Hep B) was responsible for approximately 555 000 deaths (95% UI 487 000 to 630 000) in 2019. HBV related cirrhosis was responsible for 59.6% (95% UI 50.3 to 70.6) of deaths, HBV related liver cancer was responsible for 34.6% (95% UI 29.2 to 40.4) and acute Hep B was responsible for 5.9% (95% UI 4.3 to 8.1) of Hep B related deaths.6
Overall rates of chronic Hep B are improving. Global, all age prevalence has decreased 31.3% (95% UI 29.0 to 33.9) since 1990. For children under 5, globally the prevalence has reduced by 76.8% (76.2 to 77.5) since 1990. The Western Pacific region had an impressive 93.6% (95% UI 93.3 to 94.0) reduction in under 5 prevalence since 1990. Since 1990, HBV related deaths increased by 5.9% (95% UI -5.6 to 19.2). Otherwise, age-specific DALY rates have decreased over time.
The significant declines in prevalence of hepatitis B, especially amongst children under 5, are likely linked to the scaling up of HBV vaccination in children.10 Coverage with 3-dose vaccination regimens for HBV have increased from 29% to 81% from 2000, to 2019.However there remains significant disparities globally in vaccination rates.11 The African region remains below targets with regard to vaccination rates, with less than 10% of neonates receive timely birth-dose vaccination.12
Tractability
What treatment/prevention is available for Hepatitis B?
Hepatitis B is a preventable, and treatable disease. Prevention includes vaccination, and post-exposure prophylaxis with hepatitis B immunoglobulin. Treatment of chronic infection is with anti-viral medications, which are usually continued lifelong.
Prevention
Hepatitis B vaccination and post-exposure prophylaxis with HBV immunoglobulin are both effective means of preventing CHB in infants born to HBV positive mothers. Compared to placebo, full course HBV vaccine reduced the risk of CHB in infants by approximately 72% (Risk Ratio 0.28 95% CI 0.20 to 0.40). There was no difference between 3 or 4 dose regimens. There was no difference between HBeAg positive or HBeAg negative studies included in the review. HBV immunoglobulin alone (i.e. without vaccination) reduced risk of transmission by 50% (RR 0.50 95% CI 0.41 to 0.60). Combination vaccination and HBV immunoglobulin significantly reduced the occurrence of HBV in infants by 92% (RR 0.08 95% CI 0.03 to 0.17).13
Treatment with anti-viral medication of women with HBV (peripartum antiviral prophylaxis) is strongly recommended. Anti-viral treatment reduced the risk of CHB in infants born to mothers who were HBsAg positive by 70% (RR 0.3 95% CI 0.3 to 0.4).14
Vaccination against HBV is highly cost effective. One study from The Gambia found a cost of $47 USD (2002 USD) per DALY averted.15 A modelling study which investigated the costs associated with a cold temperature chain outreach vaccine delivery model to improve acquisition of birth-dose vaccination found a cost of $0.15 to $79.72 per DALY averted from the delivery model.16 Little cost-effectiveness data is available for HBV immunoglobulin. Given it is a blood product that requires significant infrastructure and expertise at a high cost, its cost-effectiveness is unlikely to be competitive with vaccination.
A high-quality modelling study published in The Lancet Gastroenterology and Hepatology found scaling up peripartum antiviral prophylaxis to all HBsAg positive women could avert approximately 13.5 million DALYs (95% UI 12.3 million to 14.1 million) by 2100. Of these, approximately 8.3 million DALYs would averted in the African region. The cost per DALY averted ranged from $985 USD (95%UI 878 to 1128) in the African region, to $6587 USD (95% UI 5511 to 7730) in the European region.17
Treatment
Treatment of CHB is complex and guidelines vary internationally with regards to timing and choice of commencing anti-viral medication. Generally, treatment is lifelong, with <1% of individuals clearing chronic infection and being able to successfully remain off anti-viral medications.18 Treatment with commonly used anti-viral medications (e.g. entecavir and tonofovir disoproxil fumarate) can achieve viral suppression in >90% of cases.19
The cost effectiveness of anti-viral treatment varies depending on context. One cost-effectiveness modelling study found a cost of $14 590 USD per QALY gained from treatment in all HBsAg positive patients in China.20 An economic analysis from The Gambia found a cost of approximately $511 USD per QALY gained from community based screening and treatment.21
Neglectedness
Current programs/funding
The morbidity and mortality associated with hepatitis B is largely preventable through prevention and treatment efforts. Despite improvements in rates of hepatitis B, it remains the cause of significant morbidity and mortality worldwide. Hepatitis B can be considered a neglected tropical disease insofar as it:
Has the majority of morbidity and mortality borne by low- and middle-income countries where resources are inherently constrained and directed to competing health concerns such as HIV and malaria.
Disproportionately impacts populations affected by poverty, causing morbidity and mortality including stigma and discrimination.
Relatively neglected by research (i.e. resource allocation not in keeping with burden of the disease)
Amenable to broad control, elimination or eradication by applying public health strategies.22
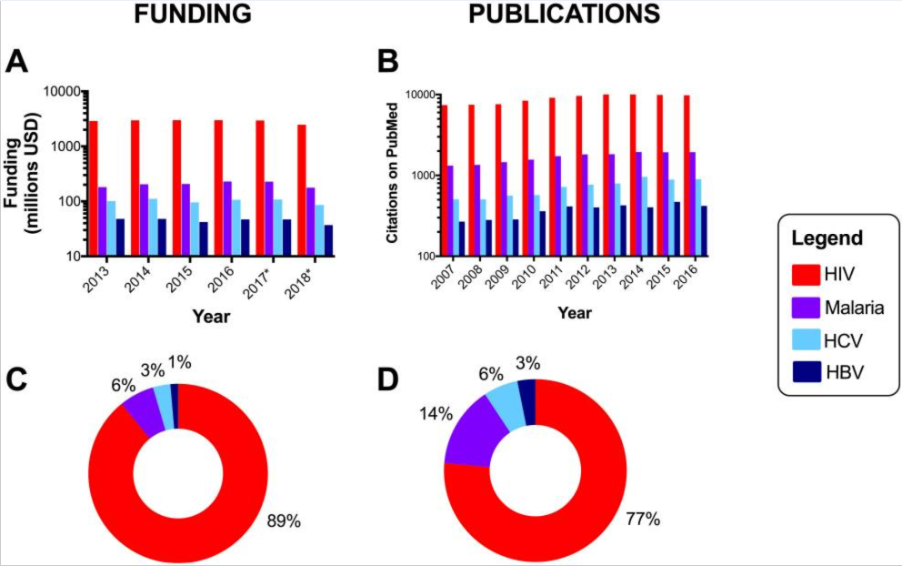
A review of expenditure on infectious disease research in the UK from 1997 to 2013 found 0.7% of total expenditure allocated to hepatitis B, 13.9% allocated to malaria, and 17.5% allocated to HIV. This is incommensurate with the relative burden from each of the respective diseases.23
More anecdotally, when conducting an initial search on Medline for a recent systematic-review on interventions to improve screening for maternal HIV, syphilis and HBV, a sensitive search approach yielded 1 288 results for HIV, 457 results for syphilis, and only 160 results for hepatitis B. This is despite HIV (all ages) resulting in 47.6 million DALYs,24 congenital syphilis resulting in 3.6 million DALYs,25 and hepatitis B resulting in 18.2 million DALYs.6
There are definite gaps in the landscape of hepatitis B, especially for interventions with proven effectiveness. Scaling up of programs to ensure antenatal screening, birth dose hepatitis B vaccination, and potentially HBV peripartum antiviral prophylaxis offer cost-effective means of addressing mother-to-child transmission. Statistics on rates of antenatal hepatitis B screening are sparse, a review from Nigeria found a screening rate of 7.2% for hepatitis B, compared with 16.3% for syphilis and 90.3% for HIV.26 Although global coverage rates for hepatitis B vaccination is approximately 80%, only 42% receive a birth dose vaccination. In the African region, the birth dose vaccination rate is approximately 17%.27 Peripartum antiviral prophylaxis, although recommended by WHO, has an estimated uptake rate of <1% in eligible women.28
References
1. Hsu Y-C, Huang DQ, Nguyen MH. Global burden of hepatitis B virus: current status, missed opportunities and a call for action. Nature Reviews Gastroenterology & Hepatology 2023: 1-14.
3. Shiffman M. Management of acute hepatitis B. Clin Liver Dis 2010; 14(1).
4. Batra Y, Acharya S. Acute liver failure: prognostic markers. Indian J Gastroenterol 2003; 22 Suppl 2.
5. McMahon B. Natural history of chronic hepatitis B. Clin Liver Dis 2010; 14(3).
6. Collaborators G. Global, regional, and national burden of hepatitis B, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Gastroenterol Hepatol 2022; 7(9).
7. Akseer N, Rizvi A, Bhatti Z, et al. Association of Exposure to Civil Conflict With Maternal Resilience and Maternal and Child Health and Health System Performance in Afghanistan. JAMA Netw Open 2019; 2(11): e1914819.
8. Yao JL. Perinatal transmission of hepatitis B virus infection and vaccination in China. Gut 1996.
9. Chevaliez S, Roudot-Thoraval F, Hézode C, Pawlotsky J, Njouom R. Performance of rapid diagnostic tests for hepatitis B surface antigen detection in serum or plasma. Diagnostic microbiology and infectious disease 2021; 100(2).
10. Cui F, Shen L, Li L, et al. Prevention of Chronic Hepatitis B after 3 Decades of Escalating Vaccination Policy, China. Emerg Infect Dis 2017; 23(5).
11. GBD Collaborators VCC. Measuring routine childhood vaccination coverage in 204 countries and territories, 1980-2019: a systematic analysis for the Global Burden of Disease Study 2020, Release 1. Lancet 2021; 398(10299).
12. Lesi O, Ward J. Paving the way towards hepatitis B virus-free generations in Africa. Lancet Glob Health 2021; 9(11).
13. Lee C, Gong Y, Brok J, Boxall E, Gluud C. Hepatitis B immunisation for newborn infants of hepatitis B surface antigen-positive mothers. Cochrane Database Syst Rev 2006; (2).
14. Brown R, McMahon B, Lok A, et al. Antiviral therapy in chronic hepatitis B viral infection during pregnancy: A systematic review and meta-analysis. Hepatology 2016; 63(1).
15. Kim S, Salomon J, Goldie S. Economic evaluation of hepatitis B vaccination in low-income countries: using cost-effectiveness affordability curves. Bull World Health Organ 2007; 85(11).
16. Scott N, Palmer A, Morgan C, et al. Cost-effectiveness of the controlled temperature chain for the hepatitis B virus birth dose vaccine in various global settings: a modelling study. Lancet Glob Health 2018; 6(6): e659-e67.
17. Nayagam S, de Villiers M, Shimakawa Y, et al. Impact and cost-effectiveness of hepatitis B virus prophylaxis in pregnancy: a dynamic simulation modelling study. Lancet Gastroenterol Hepatol 2023; 8(7).
18. Wu Y, Shen C, Chen X. Antiviral treatment for chronic hepatitis B: Safety, effectiveness, and prognosis. World J Clin Cases 2019; 7(14).
19. Scaglione S, Lok A. Effectiveness of hepatitis B treatment in clinical practice. Gastroenterology 2012; 142(6).
20. Zhang S, Wang C, Liu B, et al. Cost-effectiveness of expanded antiviral treatment for chronic hepatitis B virus infection in China: an economic evaluation. Lancet Reg Health West Pac 2023; 35.
21. Nayagam S, Conteh L, Sicuri E, et al. Cost-effectiveness of community-based screening and treatment for chronic hepatitis B in The Gambia: an economic modelling analysis. Lancet Glob Health 2016; 4(8).
22. O’Hara G, McNaughton A, Maponga T, et al. Hepatitis B virus infection as a neglected tropical disease. PLoS Negl Trop Dis 2017; 11(10).
23. Head M, Fitchett J, Nageshwaran V, Kumari N, Hayward A, Atun R. Research Investments in Global Health: A Systematic Analysis of UK Infectious Disease Research Funding and Global Health Metrics, 1997-2013. EBioMedicine 2015; 3.
24. Tian X, Chen J, Wang X, et al. Global, regional, and national HIV/AIDS disease burden levels and trends in 1990-2019: A systematic analysis for the global burden of disease 2019 study. Frontiers in public health 2023; 11.
25. Kahn J, Jiwani A, Gomez G, et al. The cost and cost-effectiveness of scaling up screening and treatment of syphilis in pregnancy: a model. PloS one 2014; 9(1).
26. Olakunde BO, Adeyinka DA, Ndukwe CD, Oladele TT, Yahaya HB, Ijaodola OA. Antenatal hepatitis B screening in Nigeria: A comparative analysis with syphilis and HIV. Int J STD AIDS 2021; 32(14): 1290-7.
28. Polaris. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: a modelling study. Lancet Gastroenterol Hepatol 2018; 3(6).
The question of how to use our resources, whether they be time or money, to contribute to the betterment of the world is difficult to answer. Any model which attempts to answer this question must consider a broad and diverse range of factors, such as unintended consequences, second-order effects and marginal impacts. For this piece I want to focus on two distinct perspectives on how one might most impactfuly use $100 000 to make a positive impact on the world. I will use a recent personal example to flesh out each perspective.
Perspective 1: The Objective position
The question of how to most effectively use one’s money or time to positively impact the world is one that the utilitarian may feel they are particularly well positioned to respond to. This is especially so when the question is posed broadly without respect to, or knowledge of, any individual actors’ circumstances or comparative advantages, or specific consequences. The feature of agent neutrality is a strength for the approach. A strict cost-benefit analytic framework may be the preferred means of ranking practical solutions when optionality exists, with a project’s benefits per unit of cost calculated, and resources allocated to the top potential projects in order to maximise the resource’s impact.
This approach is attractive for a number of reasons. It offers quantifiability and reduces the impact of personal bias. If methodology is standardised, it ideally would remove differences of opinion or concerns for corruption from a funders point of view. It would also allow for better coordination and planning for the allocation of additional resources. More detailed analysis could be extrapolated, such as calculating the marginal returns of additional resource allocation, in order to further nuance resource allocation decisions.
Perspective 2: The Subjective position
Every individual actor necessarily is influenced by a unique set of circumstances, connections, skills, i.e. their comparative advantages. This fact is important as it augments the way in which a prespecified set of resources may be allocated or used. Any two individuals may have very different opportunities in most efficiently allocating resources. As an outside observer would not possibly be able to integrate the information required to appreciate the position of the individual, evaluation of the choices made by the individual are at best a loose approximation of the actual quality of the decision. Every actor may have very different choice sets available to them. Two individuals given the same resources will likely produce very different results, even if allocating these resources based on the same principles.
This approach is attractive in different ways to the objective position. In the same way the market benefits from individualised skill and the division of labour, the use of an individual’s resources and knowledge in a way most suitable to them diversifies the approaches to how good is done. It may produce unique approaches that an outside observer would not have been able to predict. I also believe this approach provides a more ‘organic’, or bottom up, alternative to the more prescribed utilitarian approach, in that an individual’s choice has considerations for second order or unintended consequences ‘baked in’ in a way that approaches founded on reasoning and logic alone struggle to integrate.
So what is it then that I would do?
After reading Singer’s Famine, Affluence and Morality and engaging with a chunk of Effective Altruism literature, for a long time I think my answer would have been to donate the money to the Against Malaria Foundation, or one of Givewell’s other top charities. This choice would have been closely aligned with the Objective option outlined above. However, over time, my approach to this question has slowly taken a different shape.
I have included below a quote from the conclusion of Hayek’s The Use of Knowledge in Society. The paper argues for the decentralised nature of knowledge and the importance of free markets and individual actors’ use of contextual knowledge in order to forward society, or at least that is what I had taken away from it. I think there are some strong parallels to the question posed here. Whilst the Objective approach may not explicitly claim to be acting as a central theory which distributes resources in the maximally optimised fashion for a society’s improvement, it does necessarily imply some form of ‘ranking’, or superiority of the programs it suggests over alternative approaches. Implicit in this is the idea that we can somehow integrate all the relevant information and draw conclusions on actions which are likely to do the ‘most’ good in a society. Whilst concession is often made by the Objective approach that ideas beyond what is currently known may trump the suggestions that are presently ranked highly, the very idea that enough information can be integrated over time and across contexts to meaningfully capture the true ‘impact’ of a specific program or intervention seem difficult to put much credence in.
“…there is something fundamentally wrong with an approach which habitually disregards an essential part of the phenomena with which we have to deal: the unavoidable imperfection of man’s knowledge and the consequent need for a process by which knowledge is constantly communicated and acquired. Any approach, such as that of much of mathematical economics with its simultaneous equations, which in effect starts from the assumption that people’s knowledge corresponds with the objective facts of the situation, systematically leaves out what is our main task to explain. I am far from denying that in our system equilibrium analysis has a useful function to perform. But when it comes to the point where it misleads some of our leading thinkers into believing that the situation which it describes has direct relevance to the solution of practical problems, it is high time that we remember that it does not deal with the social process at all and that it is no more than a useful preliminary to the study of the main problem.”
The Use of Knowledge in Society, Friedrich Hayek
Working with a community based development organisation in rural Tanzania, we have directed funding toward two independent development projects which are highly contextual in their requirements. One is a maternal health project, specifically expanding the maternity services at the local health centre so that a full suite of antenatal and perinatal care, including surgical means of delivery, are available to women delivering in the local area. The second is a fish farming project utilising the vicinity of the project to a nearby lake and exploiting local marketable goods to generate jobs and skill acquisition for community members. Given available resources, I believe money directed toward these projects represents a ‘better’ allocation of resources than direction toward an established cost-effective intervention (such as those recommended by Givewell).
There is a higher level of certainty around the need for/likely success of these interventions
Interventions which flourish at scale require the property that they’re able to be successful independent of context. A preventative malaria campaign does require some sensitivity to local societal and cultural practices, but can quite easily be ‘layered on’ to an existing community to yield benefit. This is advantageous in that it is transferable across time and place. Interventions such as the maternal health, or fish farming project, outlined above however fall somewhat on the other end of the spectrum. They are highly context relevant. Without having formally investigated the questions, I would be surprised if attempting to scale up maternity centers to the level of being able to perform cesarean sections had anywhere near the (somewhat) uniform distribution of impact something like a preventative malaria campaign had. There is more likely to be a wider distribution of potential impact for such contextual interventions, that pivot on the need and current resource availability. The same applies for a development project such as the fish farming initiative. Would this be an appropriate intervention to apply to a wide range of developing communities? Highly unlikely. Is it worth piloting (see diversification of ideas below) in a fishing community with access to natural resources and a market for its products? It probably is.
The current emphasis for scalable programs misses potential opportunities for effective programs specific to specific communities. Of course, the main caveat to the claim of greater certainty or impact is the limitations in terms of scale. Current global-health interventions delivered at scale have an enormous positive impact on the world, but perhaps considering applying this context-specific approaches could offer a strong, complimentary, range of development interventions, which address specific needs and strengthen communities.
Diversification of ideas
Communities across the globe have diverse needs and capabilities. A focus on implementing context specific interventions is likely to derive a highly diverse set of interventions. Whilst these interventions may be highly context dependent, there is also a possibility that lessons or features can be drawn that are relevant to the development community more broadly. Perhaps an approach which seeks to address neglected and tractable issues at the community level, rather than issues which are important, neglected and tractable at the global scale, would offer greater opportunities for cost effectiveness. Generalising this principle to a variety of communities may offer an alternative approach to doing good at scale.
Opportunity to build capital/experience/skills in development work
This point is far more selfish but is a relevant consideration if one’s goal is to ‘do good’ over the course of their entire career. By utilising the $100 000 to implement specific projects, rather than making a donation to an already functioning organisation with a track record of doing effective good, there is the opportunity to be involved in and learn from a series of experiences that would otherwise be unavailable to me. The process of thinking through project implementation, monitoring and evaluation, as well as more pragmatic considerations of infrastructure development and local policies and procedures are all important and generalisable skills for a career in development.
Limitations
In writing a piece such as this there are a number of biases which ought to be highlighted and additional considerations which are important in thought around the question of an ‘objective’ vs ‘subjective’ use of resources.
Levels of intervention
The Objective approach is likely to be more useful at a high level, whilst the Subjective has its strengths in the local level where contextual knowledge is very important. Policy decisions necessarily need to consider the needs of a group rather than the individual, and thus taking a ‘subjective’ position may not be of most benefit under these circumstances. This is not, however, to say that the ‘subjective’ approach has no utility, interest groups and those who lobby policy makers on behalf of groups of individuals apply the ‘subjective’ approach to higher level decision making, and via a so called marketplace of ideas, along with representatives from other interest groups, contribute to broad policy decisions being tailored to the groups which are represented in the populous. This line of argument itself is open to all of the criticisms which are applicable to any process of democracy, but it is nevertheless an important line of thought.
Potential for corruption
In taking a subjective viewpoint and going away from more objective and evidence-driven approaches, the subjective position opens itself to the bias and faults of human decision making. This includes the propensity for individuals to become misaligned from working toward the interests of the group they seek to help, whether this may be with or without intention. Utilising the context specific personal knowledge characteristic of the subjective approach makes outside evaluation more difficult, and choices in resource allocation less transparent. This is an issue not only directly, in the sense that it is difficult to know if resources are being allocated effectively, but also indirectly, in the sense outside actors are less likely to be inclined to fund activities whose decision making is not transparent.
Difficulty in obtaining proof-of-concept
The gold standard in evidence for any intervention in the social sciences and medicine is that of the randomised controlled trial. The RCT is dependent on taking groups with similar baseline characteristics and varying only the intervention. This can mean that the effectiveness of interventions which leverage the context specific knowledge relevant to a particular community will be difficult to demonstrate using the RCT approach. Or that conducting RCT level analysis costs more than the proposed program itself. Lower levels of evidence, such as before-and-after studies may be the only reliable means of such data-gathering. Consider the maternal health and fishing interventions mentioned above. A RCT assessing the impact of holistic maternal healthcare services would be constrained by the resources required to build enough units to reach a level of statistical significance in analysis. A RCT assessing the effectiveness of a fish farming program would be difficult to interpret, unless all included study sites had similar sections of their economies dedicated to fishing. This does not however mean these programs should be abandoned, just that care and nuance needs to be applied in evaluating their impact.
Closing thoughts
I wrote this as a reflection on my own personal experiences with fundraising and involvement with global health and development work. For some time I had been convinced allocating one’s own resources, and attempting to direct others toward the most cost-effective interventions was the best means of doing good given its objectivity and perceived certainty. However as I became involved, and spent time living and working with a specific community organisation in Tanzania, I began to re-evaluate my previous framework of thinking about ‘doing good’.
I had spent some time fundraising and talking to friends and colleagues about effective giving, and had some, but little, traction. As is the way with human emotions, when I began speaking about the specific health centre I had worked in, the specific patients I had treated, and the specific issues that needed addressing, people were far more interested and excited. This directly and indirectly led to us at the Cedar Foundation raising sufficient funds for the two projects in Kamanga, Tanzania.
Specifically in regard to the maternal health and fish farming projects, the given funds were raised from philanthropic sources who made donations with less data driven and outcome contingent processes (as opposed to more evidence driven EA or EA-adjacent funders). It is unlikely these resources would have been made available to us if they had not been for projects with an attractive narrative. Considering the counterfactual scenario that these projects did not exist, the money would have likely either not been donated charitably at all, or to a local charity in a high-income setting, where these donors had previously allocated funding. I believe by helping to direct these resources into exploratory, context-specific, global health projects the potential impact may have benefits which are highly valuable for the community and us as implementors. These benefits are likely to be both direct, in treating disease and increasing economic activity locally, and indirect, in strengthening health systems and teaching us important and generalisable lessons about project implementation.
My argument here isn’t that everyone should drop the principle of cost-effectiveness, choose a community and attempt to max it out on wellbeing, but more that for an individual working toward doing good, taking a narrower frame of reference can offer opportunities and lessons that may not otherwise be available. These opportunities and lessons can both be valuable in themselves, and leveraged into further opportunities in the future. Whilst the question of what one would do with $100 000 is slightly provocative, for those interested in a career outside of earning to give, thinking laterally beyond what we see as the best buys in global health can have value well beyond the immediate impact of the project, value which should be strongly considered in making these decisions.
Prevention of global catastrophic biological risks (GCBRs) and improving global health and wellbeing are top priorities for those concerned with doing good effectively. My aim is to make the argument for a focus on health systems as a means of facilitating a broad range of cost-effective interventions, and thereby serving an avenue to, and multiplier of, potential impact for those interested in both the near- and long-term future. There are likely enough effective interventions within the space of GCBR mitigation and global health and wellbeing that would benefit from a strong baseline health system for a focus on strengthening health systems to present a robust, and diversified means of doing good. To draw a parallel from the issue of climate change, Will MacAskill in his interview with 80000 hours identified clean energy as “weirdly, robustly good”, a “win-win-win-win-win”. The wins included:
Direct health improvements from particulate reduction
Improvements for climate change
Investments in innovation speeding up technological progress
Reductions in energy poverty in low income countries
Preserving coal stores which may be needed by future generations
I believe that a focus on strengthening health systems offers similar robustness in its potential to do good, including:
Direct health improvement from access to health care
Reduction in economic costs associated with disease and infirmity
Scale up of evolving surveillance for novel pathogens
A platform from which to launch therapeutic or vaccination campaigns
The health systems approach to improving global health and wellbeing is not novel. However, in framing this approach as a means of amplifying the impact of more traditions ‘cost-effective’ interventions, I believe it is relatively neglected. The importance of health systems to the mitigation of risks from GCBRs likewise presents a relatively neglected point of view, that adds to the expected value of a health systems approach from a long-termism perspective. For those who hold high levels of uncertainty surrounding the relative importance of the near- and long-term futures, a focus on health systems could offer an approach working toward positive impact on both fronts. As such I believe focussing on health systems strengthening is a robust means of doing good, which is currently particularly neglected amongst EAs.
Strengthening Health Systems: Historical perspective
There is a long history of conflicting approaches to improving health metrics in global health. Should a broad health systems approach be used, or should we focus the limited available resources on cost-effective interventions with measurable outcomes? The Alma Ata Declaration1 at the 1978 International Conference on Primary Health Care aimed to set the trajectory toward focus on horizontal, broad health service development as a means to closing the gap on inequalities in global health. Criticised for being too broad and without actionable goals, the focus was shifted to selective primary health care (SPHC). Guided by principles of cost-effectiveness and measurable progress the GOBI-FFF strategy (programs focussing on Growth monitoring, Oral rehydration solution, Breastfeeding, Immunisation, Family planning, Female education, Food supplementation) implemented by UNICEF in 19832 provided a rebuttal, an example of a focused, and cost-effective series of health interventions that positively impacted many across the developing world. Rates of immunisation in the developing world increased from 20% to 40%, and more children than ever had access to simple yet lifesaving interventions such as oral rehydration solution.3 Whilst undoubtedly effective in achieving its goals, the approach did little in terms of bolstering the health systems of the nations it benefitted. The nature of the interventions which were invested upon meant the approach provided little foundation from which an effective, equitably distributed health system could be built.
The debate between narrow and horizontal approaches to improving health across the globe remains active to date. Whilst the amount of resources dedicated to either such approach is near impossible to aggregate,4 giving adequate thought to both the focussed (intervention specific) and broad (systems based) approaches is necessary in any meaningful discussion on how best to allocate resources within the field.
Health Systems and Cost-Effective Interventions
A comprehensive health system, sensitive to local context, with the ability to provide high-quality, timely and affordable healthcare is the utopic goal for many in global health. The World Health Organisation’s 2007 report Everybody’s Business: Strengthening Health Systems to Improve Health Outcomes makes the case for a health systems approach to achieving the goals outlined in the Millennium Development Goals, and outlines 6 building blocks of an effective health system:5
1. Health services
2. A health workforce
3. Health information systems
4. Access to medical products, vaccines and technologies
5. Health financing
6. Leadership and governance
These points are incredibly broad, and perhaps somewhat difficult to draw specific, tractable action points from. They signal the importance of institutional strength and the reliance of a healthcare system on logistics, technology, budgeting and human resources. As such, effective health sector reform is contingent on many factors, such as political considerations and public policy, environmental conditions and economic development.6 The interplay of these factors mean monitoring progress can be difficult, and the impact of interventions can be unclear. These reasons can make taking a health systems approach less appealing for those, such as EA’s, who highly value high levels of certainty in measuring and maximising impact. I believe it would be an unfortunate unintended consequence for broad interventions, with a strong theory of change, to be underutilised because they’re more challenging to evaluate quantitatively.
It is important to note that drawing a line delineating narrow from horizontal approaches to improving global health is a false dichotomy. Narrowly focussed interventions can pave the way for a broader system to be established, and a focus on health systems can make current and future cost-effective programs more efficient to implement. It is a symbiotic relationship. Given the focus on interventions with more vertical approaches, an opportunity for greater efficiency, as well as a more robust and sustainable positive impact may be achieved by turning some focus and resources toward an approach that seeks to strengthen health systems. A diagonal approach,7 one which leverages the efficiency gained by a focus on both cost-effect and narrowly focused interventions, and the underlying systems that strengthen their implementation and impact, should be the focus.
Let us consider two examples of cost-effective and impactful interventions from top EA cause areas to further explore the idea.
Malaria Prevention
In 2021, there were approximately 247 million cases of malaria worldwide, with the disease being responsible for approximately 619 000 deaths world-wide.8 Insecticide treated bed nets (ITNs) are a low cost and effective means of preventing malaria infection in endemic regions.9 The Against Malaria Foundation (AMF) is a GiveWell top rated charity,10 providing bed nets at scale, monitoring its impact, globally saving the lives of hundreds of thousands each year, and reducing the economic impacts of malaria to society more broadly.11
Considering pragmatically what is required for carrying out the programme on the ground, the AMF has a number of necessary criteria when considering areas in which to roll out ITNs for malaria prevention,12 including:
Accurate household-level data on the demand or need for nets
Independent supervision at the ‘moment of net distribution’
Post-distribution monitoring of net use and condition
Monthly malaria case rate data after distribution
Whilst there is no specific requirements for established health care system architecture to be in place, the AMF does stipulate the following considerations in evaluating potential partners:12
· Would the National Malaria Control Programme (NMCP) agree to the four main requirements we have of a distribution?
· Are there potential distribution partners with the necessary resources and experience with whom we could collaborate?
· Is there a strong leader in charge of the distribution partner(s) with whom we feel we can work closely?
Consider two alternative scenarios, one in which the AMF ITN program is run in partnership with a local health centre offering contextually appropriate primary care (scenario A), and one in which the program is run in partnership with an organisation meeting only the minimum essential requirements (scenario B). For the narrow purposes of malaria prevention, scenario B is likely to be the more cost-effective of the two. Costs will not need to be distributed across competing priorities, and the program can optimise for data collection, net distribution, and outcome evaluation. If we consider a broader view of the overall health of the community, there are a number of factors that favour the effectiveness of scenario A, despite a likely higher cost. The efficiency of the ITN program implementation is likely to be greater given availability of basic resources such as brick and mortar infrastructure, and the ability to communicate the occurrence of the program to the local community. The uptake of the program may be more acceptable in a community where the local health centre is a trusted and integrated resource the community regularly utilises. There will be opportunity for gains to be made from educating the community about malaria. Community members may have a greater awareness of signs or symptoms of the disease and be more likely to present to the health centre and complete treatment in the future. Data collection of future cases of malaria may be more robust in a setting where the data collection and treatment point are the same physical location. Importantly, these benefits are more dispersed in time and place than those of the leaner scenario B, and as such are more difficult to quantify and integrate into a cost-effectiveness analysis. This should however not detract from its benefits, measured or not, they do exist. As such, I believe there is a strong argument to be made for a synergist approach in which the impact and sustainability of cost-effective, narrowly focussed public health interventions is supplemented and amplified by an underlying health system infrastructure.
Genomic Surveillance for Prevention of GCBRs
Emerging novel pathogens or the spread of high consequence existing pathogens pose an existential threat to humanity, and we as a species have an interest in their early detection, and in a prompt response to potential threats. These pathogens pay no attention to political lines or nation states and thus, technological strategies cannot be isolated to reference laboratories in high-income nations, they must necessarily be present globally. A wide variety of approaches exist to mitigate the potential consequences of GCBRs. Early detection of novel pathogens, broad spectrum therapeutics or vaccinations and quarantine facilities are all potentially useful and impactful means to reducing the existential risk associated with GCBRs. At each of these steps, there is a potential dependence on an underlying health infrastructure, a platform from which pathogens can be detected, therapeutics can be dispensed, and individuals can be quarantined. In a similar fashion to the argument outlined above, the ability to leverage an existing health system to implement a wide variety of mitigation approaches to GCBRs seems like a robustly good approach to doing good.
As an example, pathogen agnostic genomic surveillance systems have been suggested as a global public health priority in reducing the risk from pathogens with pandemic or epidemic potential. Pathogen agnostic systems survey biological data across a geographical region, screening for genomic patterns suggestive of an emergent or novel disease. A recent strategy report from the WHO outlines objectives required to achieve the goal “that genomic surveillance for pathogens with pandemic and epidemic potential is strengthened and scaled for quality, timely and appropriate public health actions within local to global surveillance systems.” The objectives are as follow:
Improve access to tools for better geographic representation
Strengthen the workforce to deliver at speed, scale and quality
Enhance data sharing and utility for streamlined local to global public health decision-making and action
Maximise connectivity for timely value-add in the broader surveillance architecture
Maintain a readiness posture for emergencies
Objectives 1, 2, and 5 are obvious candidates for greater efficiency if an underlying healthcare architecture is available. In a setting where resources are already limited, there may be an obstructively high bar to the proper implementation of a genomic surveillance system, which could at least partially be overcome by the presence of the architecture of a health system. In LMICs without centralised sewerage systems, surveillance of biological materials may prove difficult if not carried out in the context of a health centre or dispensary, where respiratory swabs, urine, or faecal samples could be collected and analysed at the point of care. A readiness posture for an epidemic or pandemic similarly, will require human resources and likely be more effective if a locally, contextually effective health care system can be leveraged to deliver such an escalation plan.
Actioning a health systems approach
By nature, a ‘health systems’ approach is broad and as such can encompass a variety of potential areas of focus. Taking such an approach should not ignore arguments of cost-effectiveness, cost-effectiveness should remain an important means of arguing for the prioritisation of specific interventions within this approach. Utilising the 6 building blocks identified by WHO, we have a reasonable breakdown of potential focus areas that are somewhat more specific and actionable. I have included some brief thoughts on potential actionable areas for action within each of the building blocks:
Health services
In actioning a health systems approach, a primary focus may be on establishing and enhancing primary healthcare infrastructure, especially in regions with significant needs or geographical isolation. This could involve investments in the fundamental requirements for primary care delivery, such as facilities, equipment, and necessary medications (including vaccinations). Additionally, exploring innovative care delivery models, such community-based investigation and treatment for prevalent diseases (e.g. HIV, TB, antenatal syphilis or hepatitis B), can lead to more efficient and effective healthcare services. Evaluating these novel models through research can provide insights into their scalability and replicability in different contexts.
Example: A systematic review by Vaughan et. al. has suggested utilising community health worker (CHW) programs for the delivery of tuberculosis treatment and control, reproductive and child health, and malaria interventions can be more cost effective in comparison to standard care.
A health workforce
Addressing the health workforce involves ensuring accessible education and training avenues for potential health staff in areas of need, such as, for example, remote learning opportunities for aspiring community health workers. Ensuring there are not undue barriers to the training of health staff, and a focus remains on pragmatic requirements for healthcare delivery, (e.g. low-cost options or scholarships for those seeking specialists training from areas of need), is essential. Additionally, incentivization strategies for health workers, like scaled remuneration or other benefits for those serving in remote regions, can address the issue of workforce shortages in critical areas.
Example: A systematic review by Callaghan et. al. found ‘task-shifting’ interventions, the deligation of routine and repetitive tasks from doctors to non-physician clinicians, in HIV treatment and care was a cost-effective means of delivering high-quality and more cost-effective care tose living with HIV in sub-Saharan Africa.
Health information systems
Investment in digital healthcare infrastructure is an important aspect of a strong health system, emphasising efficient data management and sharing, such as centralised reporting systems for notifiable diseases. Moreover, the development and implementation of surveillance systems for novel pathogens are vital in developing health systems, particularly as pathogen-agnostic diagnostic technologies become more affordable. Ensuring the rollout of these technologies in low- and middle-income countries can significantly enhance global disease monitoring capabilities.
Example: An observational study by Secor et. al. highlighted the potential added value of scaling electronic immunisation registries, looking at data collected from a program in Tanzania, with the potential to improve vaccination rates, identify populations at risk for disease and improve care delivery more broadly.
Access to medical products, vaccines and technologies
Developing robust supply chains is essential for the distribution of key equipment, vaccinations, and medications. This can include monitoring systems for stock-outs of crucial diagnostic tests and essential medications. Investment in research and development of supply chain management can also play a significant role in ensuring consistent access to medical products in diverse healthcare settings.
Example: A mixed-methods study by Lavtepatil and Gosh explored the effectiveness of the Pradhan Mantri Bhartiya Jan Ausadhi Pariyojana program, a program seeking to increase the availability of essential medications through the local production and procurement of unbranded generic medications. Whilst work there remains room for optimisation, the approach shows some promise in reducing healthcare expenditure on drugs.
Health financing
A key aspect of health financing is ensuring individuals are protected from catastrophic costs associated with healthcare, advocating for universal health coverage systems in developing economies. Furthermore, making sure that highly cost-effective interventions are cost-free or actively incentivized can lead to more equitable and widespread access to essential healthcare services (this is already a focus area for some EA focussed charities).
Example: The introduction of a community-based health insurance scheme, the Mutuelles program, in Rwanda, where subscriptions of varying premiums are paid by households, with the remainder of the funding being pooled from various NGOs, government funding or development partners. Lu et. al. found the intervention to be an effective step toward universal health coverage.
Leadership and governance
Efficient collaboration between various sectors, such as public and private health systems or NGOs, especially in regions where multiple systems coexist, is important in developing health systems. Working towards a cohesive and integrated approach can optimise resource utilisation and improve overall health service delivery.
Example: Kenya has trialled a decentralised means of healthcare governance, aiming to enable more localised decision making processes catering to regional health needs. A systematic review by Masaba et. al. found there were improvements to the development of the Kenyan health system as a result of the policy, however, did identify a number of key challenges with its implementation.
Again, none of these strategies are particularly novel or ground-breaking in and of themselves. However, given the broad potential good they can facilitate, a greater focus on strengthening these key aspects of health systems should receive greater attention for those aiming to do good in the near- or long-term.
Limitations
Neglectedness
Some may consider that a health systems focus is already the focus on many players in the global health landscape. For instance, local government bodies are likely to already be contributing resources to the elements of health system development, rather than focussing on more specific interventions that are particularly important, tractable, and neglected. The comparative advantage of an actor in the global health and development space may therefore have a large marginal impact focussing elsewhere. An argument may also be made that health systems emerge as a result of economic development, and as such in developing nations the most effective means of improving health systems is by supporting development more broadly. In rebuttal to these points, I believe that those with a lens toward doing good effectively in both the near- and long-term, could have an impact on shaping this progress with a particular focus on a more cost-effective bent. For instance, an actor with a specific concern for the risks of GCBRs could advocate for the inclusion of pathogen monitoring systems in developing health systems.
Complexity of approach
Given the interdependence of health systems on other aspects of society, and the required sensitivity to local context, two potential issues may arise:
1) Difficulty in accurate monitoring and evaluation
2) Difficulty in rapid scale up and ability to absorb funding
These are precisely the points which more narrow and quantifiable approaches to issues in public health have their strengths. In response to these points:
1) Difficulty in monitoring and evaluation does not mean the actual impact of such projects does not exist. This is an issue of monitoring and evaluation methodology, rather than program failure.
2) The development of health systems is highly contextual and resource intensive, as mentioned above. Whilst this is true, given the broad array of potential avenues to positive impact, the benefit here still outweighs these potential costs.
Opportunity cost
Numerous cost-effective programs exist outside this space with no reliance on an underlying healthcare delivery platform. It is difficult to directly compare the utility of allocating funds toward what may be considered more certain avenues for impact, rather than a high-level systems-based approach. Systems based approaches are also likely to have their impact over longer time horizons. As such, one may prefer to allocate their resources to more ‘certain’ routes of positive impact, from a traditional expected value point of view.
Conclusions
For those concerned with doing good in the near- and long-term future, global health and wellbeing, and mitigating risks from GCBRs are key issues of concern. Historically, the discourse on progress in global health has fluctuated between vertical and horizontal approaches. Arguments for progress from a cost-effectiveness point of view tend to favour vertical approaches. I argue that by taking a traditionally horizontal, or health systems approach, one can robustly contribute to progress on global health and wellbeing, and mitigating risks from GCBRs, with a reasonable level of confidence. Whilst this approach is not without its own limitations or difficulties, and noting that the two approaches are mutually beneficial, I believe the health systems approach is a relatively neglected stance taken by those concerned with doing good effectively.
References
1. Decleration of Alma-Ata. International Conference on Primary Health Care, Alma-Ata, USSR: World Health Organisation; 1978.
2. Cash R, Keusch G, Lamstein J. Child health and survival. The UNICEF GOBI-FFF program. Beckenham, UK: Croom Helm Ltd.; 1987.
3. UNICEF. 1946-2006 Sixty Years for Children. New York, NY USA, 2006.
4. McCoy D, Chand S, Sridhar D. Global health funding: how much, where it comes from and where it goes. Health Policy and Planning 2009; 24(6): 407-17.
5. Everybody’s business — strengthening health systems to improve health outcomes: WHO’s framework for action: World Health Organization, 2007.
6. Kim J, Porter M, Rhatigan J, et al. Scaling Up Effective Delivery Models. In: Farmer P, Kleinman A, Kim J, Basilico M, eds. Reimagining Global Health : An Introduction: University of California Press; 2013.
7. Ooms G, Van Damme W, Baker BK, Zeitz P, Schrecker T. The ‘diagonal’ approach to Global Fund financing: a cure for the broader malaise of health systems? Globalization and Health 2008; 4(1): 1-7.
8. World Malaria Report 2022: World Health Organisation, 2022.
9. Pryve J, Richardson M, Lengeler C. Insecticide‐treated nets for preventing malaria. Cochrane Database of Systematic Reviews 2018; (11).
A 40 year old male presents to the emergency department with shortness of breath, swelling in his legs, feeling generally unwell. He is not sure exactly when he last felt himself, but certainly for the past few weeks he has not been able to take his children out to ride their bikes or keep up with the gardening at home. The doctors in the emergency department scratch their heads, concerned, questioning him about his medical history. After a series of investigations, being reviewed by multiple medical specialists and many long and emotional conversations, he is diagnosed with dilated cardiomyopathy and acute heart failure. The diagnosis carries with it a poor prognosis, without a heart transplant, the quality and quantity of his life are likely to be reduced significantly. More tests, more specialists, and more difficult conversations take place. He is listed for a heart transplant. The waiting game begins. He lives in anticipation, waiting for the call telling him a donor has been found. The call comes, a Friday morning just after his kids have caught the bus to school. His wife rushes home, and he is whisked off. Mere hours later he waits in the anaesthetic bay nervously. His life is about to be changed forever.
Across the globe on the same morning a mother nurses her child. She is sick, she has been for about a week now. Undulating fevers, increasingly pale skin and lethargy have transformed her daughter from the little girl chasing chickens around the yard, to a docile vulnerable child battling a microscopic war within her own body. She takes her daughter to the health centre, some two hours walk away, swaddled in cloth to her back. By the time they arrive her daughter is listless. A rapid malaria test is positive. As is a urine test for protein. She has severe malaria, and her kidneys are taking a hit. The clinical officer on duty searches for a vein, and vein, to insert an intravenous line to administer the antimalarial drugs and antibiotics she needs to stay alive. She is admitted to the ward. No specialists arrive, there are no more investigations. The sun sets, and rises again the following morning. The woman sobs, as her daughter’s breathing becomes irregular, then stops. Her life is changed forever.
A heart transplant exemplifies just how far modern medicine has brought us. From the medical science necessary to surgical excise and implant the vital organ from one person to another, to the logistical challenges of coordinating the transport of the organ from donor to recipient, every heart transplant attests to just what humanity is capable of if we set our mind to it. It is also incredibly resource intensive. The pre-transplant workup, admission for transplantation, follow-up and management of complications present a significant volume of work. One US review of heart transplantation and mechanical assisted pump devices (LVAD) usage estimated a combined cost of $2.5 billion USD for the period 2005-09, with 9369 transplants and 6414 LVAD procedures taking place, placing costs at ~$158 000 per episode (1). These costs accounted only for the inpatient episode of care, excluding initial workup, and post operative care. An Australian review of pediatric heart transplantation calculated the mean cost of heart transplant at $278 480 USD (95%CI $219 282 – 337 679 USD), with follow up costs quoted at $55 823 USD (95%CI $47 631 – 64 015 USD) for the first year, and $12 119 USD (95%CI $8 578 – 15 661 USD) for each following year. The cost per QALY gained was calculated at $29 161 – 44 481 USD (2). The 1 year survival post heart transplant is 84.5%, and 5 year survival is 72.5% (3). The quality of life amongst surviving heart transplant recipients seems to be similar to that of the background population (4). Median survival post transplant is approximately 12 years (5).
In addition to the costs of the procedure and care required directly to the patient, there exists additional reservoirs of cost. For instance, significant biomedical research is necessary as a precursor to the procedure of transplantation being physically possible. Surgical technique, complex immunosuppressive regimens and perfusion systems have all had to be developed for the purposes of successfully carrying out the procedure. Or consider the infrastructure which provides support for the logistics of the transplantation. It must be operative 24 hours a day, and requires staffing from specialist medical and nursing staff. Cost estimates accounting for the direct costs associated with an individual patient’s care fail to account for the significant and costly foundation this care is based upon.
Many high-income countries are willing to invest in heart transplant services, with around 5000 transplants occurring across the world every year. Thresholds quoted by national governments for what constitutes a cost-effective intervention vary worldwide, the US has a threshold of approximately $50 000 USD per QALY gained. From the cost perspective of the individual patient encounter, the investment for each QALY for a heart transplant patient is cost-effective. This is where most analyses stop, and where our policy decisions draw the line in terms of evaluation. What would be our view on the cost effectiveness of a heart transplant if we considered all of the investment they have brought us to the point of being able to successfully add some 12 years of life to each beneficiary of the process? With some 3500 transplants being performed a year, and assuming a quality of life comparable with the background population, the efforts and investments associated with heart transplantation offer 42 000 QALYs to patients every year.
To put these 42 000 QALYs in a more global context, consider the years of life lost (YLL) associated with malaria across the world each year. According to WHO estimates in 2019, 30 855 000 years of life were lost due to malaria alone (6). 95.5% of YLL were on the continent of Africa. Findings from the Gallup World Poll suggest a positive relationship between life satisfaction and income, with members of high-income countries reporting satisfaction levels between 6 and 8, and members of low-income countries reporting satisfaction levels between 3 and 5.5 (7). Let us therefore assume, as a conservative estimate, for each absolute YLL to malaria 0.5 QALYs are lost. There are therefore some 15 427 500 QALYs lost to malaria every year. This is the same number of QALYs as are produced from more than 367 years of heart transplantation. GiveWell’s cost effectiveness analysis suggests that a death from malaria can be prevented for as little as $3 845 (8). This is far cheaper than the $29 000 – $44 000 cost per single QALY gained from a heart transplant. How then can we justify as a society the investment, costs, and opportunity costs associated with heart transplantation, given the availability of interventions, such as malaria prevention, that are so much more cost effective, and so much more vast in terms of scale?
There are a range of potential justifications for the practices of high-income countries and expensive, innovative medical treatment more broadly. Let us consider a few such justifications, and in doing so appreciate some of the complexities involved in performing this style of moral calculus:
The intrinsic value of innovation: A heart transplant represents the pinnacle of human progression. The broader trajectory of society toward healthier, happier and longer lives built on the foundation of scientific progress is nowhere more aptly exemplified than in the procedure of transplanting a human heart to give an identifiable individual another shot at life. Innovation in the broadest sense is valuable to all, albeit to some more than others, and in acting out innovation for the benefit of an individual, all involved have a tangible sense of connection to the good society has produced.
Spillover effects: Connected to this may be arguments around the interconnectedness of health progress, how innovations in one area may benefit those in adjacent fields. Could a heart transplant give us insights about the management of cardiovascular disease, which may benefit the increasing numbers of those being burdened by similar conditions in low and middle income countries?
Potential for cost reduction: Whilst innovative treatment modalities may be expensive initially, by accepting a high initial cost we are accepting the likelihood of lower costs in the future, improving the cost effectiveness of effective treatments over the long term.
Moral prioritisation of one’s own community: Many believe in the moral obligation toward those of their own family, community, and country. This may involve ideas of reciprocity, or more common-sense-morality related to the connection shared with those around them, and the direct observability of their impact. We may feel that although a heart-transplant is resource intensive, at least we can be more convinced these resources are being utilised for a qualitatively ‘positive’ purpose.
Local economic considerations: A heart transplant is a complex undertaking that not only requires the input of specialist knowledge, but the labour of many non-specialised workers. The economic remuneration from undertaking the procedure benefits all involved, whether directly or indirectly, and contributes some part to economic activity in society.
Conclusion
A bias exists toward innovative activities that in our society is morally and economically acceptable. On closer examination, it appears that a bias toward innovation and common sense morality underlies our current resource allocation. If what we truely seek to optimise is the health and wellbeing of all people, we would be wise to shift our focus from the margins of what is humanly possible, to innovation that ensure the basic needs of all people are met
References
Mulloy DP, Bhamidipati CM, Stone ML, Ailawadi G, Kron IL, Kern JA. Orthotopic heart transplant versus left ventricular assist device: a national comparison of cost and survival. J Thorac Cardiovasc Surg. 2013 Feb;145(2):566-73; discussion 573-4. doi: 10.1016/j.jtcvs.2012.10.034. Epub 2012 Dec 13. PMID: 23246055; PMCID: PMC3707397.
Ye XT, Parker A, Brink J, Weintraub RG, Konstantinov IE. Cost-effectiveness of the National Pediatric Heart Transplantation Program in Australia. J Thorac Cardiovasc Surg. 2019 Mar;157(3):1158-1166.e2. doi: 10.1016/j.jtcvs.2018.11.023. Epub 2018 Nov 16. PMID: 30578063.
Lund LH, Edwards LB, Kucheryavaya AY, Benden C, Christie JD, Dipchand AI, Dobbels F, Goldfarb SB, Levvey BJ, Meiser B, Yusen RD, Stehlik J; International Society of Heart and Lung Transplantation. The registry of the International Society for Heart and Lung Transplantation: thirty-first official adult heart transplant report–2014; focus theme: retransplantation. J Heart Lung Transplant. 2014 Oct;33(10):996-1008. doi: 10.1016/j.healun.2014.08.003. Epub 2014 Aug 14. PMID: 25242124.
Politi P, Piccinelli M, Fusar-Poli P, Klersy C, Campana C, Goggi C, Viganò M, Barale F. Ten years of “extended” life: quality of life among heart transplantation survivors. Transplantation. 2004 Jul 27;78(2):257-63. doi: 10.1097/01.tp.0000133537.87951.f2. Erratum in: Transplantation. 2012 Aug 15;94(3):e22. Poli, Paolo Fusar [corrected to Fusar-Poli, Paolo]. PMID: 15280687.
Khush KK, Cherikh WS, Chambers DC, Goldfarb S, Hayes D Jr,, Kucheryavaya AY, Levvey BJ, Meiser B, Rossano JW, Stehlik J; International Society for Heart and Lung Transplantation. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-fifth Adult Heart Transplantation Report-2018; Focus Theme: Multiorgan Transplantation. J Heart Lung Transplant. 2018 Oct;37(10):1155-1168. doi: 10.1016/j.healun.2018.07.022. Epub 2018 Aug 10. PMID: 30293612.
Deaton A. Income, health, and well-being around the world: evidence from the Gallup World Poll. J Econ Perspect. 2008 Spring;22(2):53-72. doi: 10.1257/jep.22.2.53. PMID: 19436768; PMCID: PMC2680297.
As we progress through life, we must inevitably navigate through crossroads, moving down the path of life and necessarily leaving opportunities behind. At each moment when the choice is made, a path goes on unrealised. But more than this, the person you may have been had you taken that path fades into non-existence. It is strange to think about the mourning of a person who has not yet existed, although we do do it. We mourn the loss of a child who had life still left to live, no least because of the fact there are times ahead they’re going to miss. The mourning from an unrealised path differs from a child dying in both quality and quantity, but mourning for the future is common to both. For ourselves, we often attach ourselves to a vision of who we may be in the future. When we make a decision that forces us down a certain path, that future version of us is sentenced to an unrealised existence.
The situation of a forgone path of course exists within the bounds of controllable, as well as uncontrollable circumstances. Perhaps a chance accident occurs, and we are rendered without a leg. The future we imagined running marathons or playing football in now significantly changed. In addition to the direct pain and shock of the situation, this is likely to account for some significant part of the distress associated with significant and uncontrollable life events. What is on the other side may be unexpected, and on balance, it may even be good. The proverb of the Chinese farmer offers some insight into this line of thinking:
A farmer and his son had a beloved stallion who helped the family earn a living. One day, the horse ran away and their neighbours exclaimed, “Your horse ran away, what terrible luck!” The farmer replied, “Maybe so, maybe not. We’ll see.”
A few days later, the horse returned home, leading a few wild mares back to the farm as well. The neighbours shouted out, “Your horse has returned, and brought several horses home with him. What great luck!” The farmer replied, “Maybe so, maybe not. We’ll see.”
Later that week, the farmer’s son was trying to break one of the mares and she threw him to the ground, breaking his leg. The villagers cried, “Your son broke his leg, what terrible luck!” The farmer replied, “Maybe so, maybe not. We’ll see.”
A few weeks later, soldiers from the national army marched through town, recruiting all the able-bodied boys for the army. They did not take the farmer’s son, still recovering from his injury. Friends shouted, “Your boy is spared, what tremendous luck!” To which the farmer replied, “Maybe so, maybe not. We’ll see.”
The unpredictability of the time frame within which we assess the outcome of a situation plays a pivotal role in whether we see it as favourable or not.
One other factor divides controllable against the uncontrollable pivot point, that of control itself. When the situation is in our control, we are liable to regret. We are the agent responsible for the direction taken. Regret exists as an important consideration in addition to the outcome itself. The fear of regret itself may play an important role in stalling our decision making around key life choices. Regret may itself be an inevitable feature of making such decisions, as by making a choice we necessarily forgo some other choice, which no matter how marginally positive it may be, we are liable to regret forgoing.
The ‘path’ analogy to decision making in life does require some further nuance. When choosing a path, we ideally take one which leads to a life in which we’re realising some sense of self we currently perceive as desirable. There are however two main moving parts in this equation:
The path itself is likely to take unexpected turns, be liable to change and open to some degree of malleability, i.e. paths are rarely straight, narrow and unchangeable
What we see as desirable is likely to change over time
Point 1 is exemplified well by the proverb of the farmer above. Ultimately, how we view the outcome of a choice depends upon the point at which we view the choice. If we decide to train for a long and challenging hike, we’re likely to encounter early mornings, difficult times and ultimately that at any one moment it may be preferable to stay at home and enjoy a movie, than get out and train. However, from the point of view of the person who has completed the hike, the benefits stand tall above the cost of the journey, and we can be ultimately glad we made the decision to do it.
Point 2 is more difficult to deal with. How are we to make value judgements if we’re inherently uncertain about the values upon which the judgements are based? The temptation may be to err toward optionality, making a decision that allows for maximal flexibility so that future decisions have a wider array of possibility, and account for likely future changes in values. But this isn’t particularly helpful, as meaningful paths can often require some investment of time over a prolonged period, and whilst preferring not to ‘lock in’ to a path early is understandable, it does relieve from the fact high value options exist down narrow paths. Similarly, ignoring the fact our values are likely to change over time is not productive, it’s important to attempt to anticipate the trajectory of value changes and plan accordingly. Unfortunately there doesn’t seem to be a reliable or concrete means of doing so, so where to from here?
A reasonable approach seems to be attempting to project your value set accounting for the phenomena of regression to the mean. Are there important life events you foresee arising in the next decade, or two? How will these alter your values? This is a simple and relatively intuitive approach. In addition, are you particularly on an upper or lower bound for a particular trait at the moment? Perhaps conscientiousness at work is currently a priority, and you rank somewhere near the top percentiles of the bell curve. It would be prudent to assume that your willingness to continue valuing conscientiousness at work will regress to the mean over time as your values shift. Another reasonable guiding principle is to approach the direction of one’s life with curiosity and a willingness to change one’s mind with the availability of new information or understanding. Perhaps a framework of thought and value takes some years to come to, but is sufficiently convincing to err you toward a new path in life. In order to begin down said new path, new foundations and groundwork may need to be laid, but if you’re convinced of your value set, this should just be a matter of doing the work.
“He who has a why to live for, can bear almost any how”
Friedrich Nietzche
The course of life is unpredictable, uncertain and marches forward with unrelenting fortitude. As humans we aspire to shape our lives in certain way, to mould our experience and perceptions of self. In doing so, we must forgo the opportunity to embody certain versions of ourself, to pursue the life we ultimately end up living. Navigating such a life is difficult, but there is nothing more human than doing so. The beauty is in the struggle.
In life we often strive for the philosophical, the reasoned approach, the thoughtful decision, the meaningful action. A picture of a contemplative life, to me at least, reflects the life well lived. A person who acts with purpose from a structure of well reasoned values in the world the constantly seeks to further understand, seems like the kind of person one should reasonably strive to be. Throughout their short time on this earth, exploring the depths of what it is to be human, how it is we can know anything at all, and why something, rather than nothing exists in this universe we call home. In essence, the contemplation of philosophy is the ultimate achievement of human creativity, an end of the utopian society, and an act toward which we all may strive.
From a naive view, one may question how people can go about a life in pursuit of seemingly arbitrary topics of investigation give this grand narrative. How is it that one can spend a life dedicated to the identification of insects, when questions of moral realism linger unanswered?
How can one commit to refining the culinary techniques required to produce a masterful and unique dish, when the possibility of parallel universes remains open? Are there not more pressing issues, are there not more interesting topics to which one can dedicate their life?
The first consideration is one of practicality. Whilst it would be wonderful if we could all sit around and pontificate our days away, most people in this world simply need to act practically in order to eat, remain in safe shelter, and keep healthy. The second consideration is one of preference, for some, these considerations are simply too abstract and hold no intrinsic interest as they do not impact the day to day existence they inhabit. Let us for the moment pass these two considerations, and imagine a somewhat utopian existence in which individuals are free to explore the objects of their desire.
In this world, I believe, we all would pursue philosophical ends. The entomologist continues to study insects, the chef continues to refine her art. These acts go beyond what may be considered by the outside observer. Yes, insects are of interest themselves. They’re strange creatures. But what does the study of their lives, their various forms and functions reveal to us about the world? We consider their behaviours, and reflect on the influence of the environment on all living creatures, ourselve inclusive. We think of their myriad types, many likely undiscovered, and sit in awe of the complexity and vastness that exists within our small corner of the universe. The chef, too a philosopher, explores aesthetics. What is beauty? How can a story be conveyed without words, and how does the experience differ for each individual seated eating their food? The distance runner searches for an expansive sense of self, connecting to the world around them in new and unique ways as they push the physical boundaries of fatigue. Which is the real world, the one he experiences at kilometre one, or at kilometre fourty?
Whilst academic and direct philosophical pursuits offer a direct means of grappling with the philosophical questions that characterise our very human lives, there are countless ways in which each and every person challenges these uncertainties every day. If utopia is a world in which the pursuit of contemplation is carried out as an end in and of itself, perhaps we would do well to recognise it seeping through, each and every day, in the world around us.
“A map of the world that does not include Utopia is not worth even glancing at, for it leaves out the one country at which Humanity is always landing. And when Humanity lands there, it looks out, and, seeing a better country, sets sail. Progress is the realisation of Utopias.”
Oscar Wilde
The history of humanity thus far has been vanishingly short. As a species, we are some 300 000 years old. The universe is some 13.7 billion years old. Humans have existed for 0.002% of the history of our known universe. What is even more astounding is how human life has changed over this relatively short time frame. We have progressed from existing as hunter-gatherers, to living in organised permanent settlements. Civilisations have risen, and fallen. We have farmed, industrialised and globalised. Over the past ~300 years, the number of humans living on the earth, our understanding of science, and development of technology, have all seen growth orders of magnitude greater than what we have known in the past.
Our world today is far from perfect. Disease, conflict, and inequalities exist across the globe. But it is also true that as a global community we are richer than ever. In highly developed economies, such as England, GDP per capita has shown almost uniform exponential growth over the past 300 years.
In William MacAskill’s new book, What We Owe The Future, he gives the following apt summary:
“We face massive problems today, and the world is full of needless suffering, but in some ways we have made remarkable progress over the past few hundred years. Three hundred years ago, the average life expectancy wasless than 40 years; today,it’s over 70. More than80 percentof the world lived in extreme poverty; now just around10 percent does. Women were, for the most part, unable to attend universities, and the feminist movement didn’t exist. No one lived in a democracy; nowover half the world does. We’ve come a long way.”
We have made incredible progress, in such a short period of time.
If one were to have been asked, what does utopia look like, in the year 1500, what may they have given as a reasonable answer? The ability to illuminate any room at the flick of a switch (invented by Humphry Davy in 1809)? The ability to heat any living space, at any time (electric heater invented by Thomas Edison in 1883)? Or what about the ability to see and speak with, in real time, a loved one across the globe (invented by Bell Telephone Laboratories in 1959). What about the improvements in our life expectancy, clean drinking water, and hygiene and sanitation service? Or freedom to express one’s ideology, religion or worldview, free from persecution? It would not be a stretch to consider for much of human history, the conditions of a high income, democratic society, are within the bounds of what may have been considered ‘utopian’ for the vast majority of history.
This is probably also the case for many living in absolute poverty within our modern society. If asked what utopia would look like, many of the above examples may apply, except for the fact we live in the same time and that these technologies are unavailable for economic reasons. A world in which electricity is a luxury, and one in which lights are remotely changed to an appropriate hue to suit a residents preferences, do exist simultaneously today.
Visions of utopia from a modern day perspective necessarily do require some level of progress from our current existence, at least for most. Holden Karnovsky outlines a spectrum of what utopia may look like. For instance a world which reflects our current existence, with the exception that cancer does not exist may give a conservative example of a potential utopia. From a more radical perspective, utopia may look like a world of digital people experiencing constant pleasure, free from material needs and boredom. Thinking through possible examples that exist throughout the spectrum reveals the unlikely fact that anywhere actually exists along this spectrum that is mutually acceptable to all of humanity. Instead, we are likely to continue to iterate toward a world in which society makes an interesting, valuable and value driven life available to a large fraction of people.
Where are we to draw the line given this conception? Is a society in which individuals spend money and time pursuing goods that are ends in and of themselves close to what may be considered utopia? I think that qualitatively, utopia does indeed exist for at least part of the world’s population. It exists in public parks, large art installations, and leisure time spent working on cars or attending concerts. It manifests in the free and safe lives led by people from all manner of racial, religious, gender and geographic background living lives of autonomy and free expression. In trips to the beach, and lingering conversations after a shared meal. As we continue to progress as a global society, the trend toward greater quantity, availability and depth of utopia will be the ideal toward which we should strive.
Quantity
As we technologically progress, and the availability of automation for many tasks undertaken by human becomes more of a reality, we would do well to direct this more efficient generation of goods and services, the reduction in costs and increase in free time toward meaningful ‘human’ pursuits. Perhaps a standard work week would be able to be reduced from 5, to 4 and then to 3 days, with a greater emphasis placed on pursuit of personal projects.
Availability
The availability of a utopian life in our current world is distributed in an incredibly inequitable fashion. Meaningful effort and resources should be directed toward aiming at a widespread availability for involvement in utopian society, for all humans. Much ink has been spilt on effective aid, resource distribution and addressing inequalities, we would do well to ensure this is a front-of-mind consideration in working toward utopia.
Depth
For example, a world in which individuals’ freedom and rights are restricted for demographic or other reasons is most certainly not a utopia for those individuals. The world is more utopian for removal of discriminatory practices in our societies, but there is still much work to be done. Even in societies that may qualitatively experience some aspects of utopia currently, the degree of this could be increased. This could also occur as the result of improving technologies, such as virtual reality, improved prosthetic limbs for amputees, or higher-quality public goods.
In summary, I believe utopia does exist in some fashion in parts of the world today. Whilst we certainly can and should aim to improve the world we live in, we should give considerable consideration to how we do so, and who will benefit from these improvements. This framing of utopia being available to some of us is also cause for celebration, and appreciation if one is fortunate enough to be able to benefit from the progress made by the previous 300 000 years of human history. Go to a park, swim in the beach, laugh with friends, we already live in utopia.
The economic value of a life, or value of a statistical life (VSL), is a dollar amount that an individual or society is willing to pay for the purpose of avoiding the mortality of one individual. A controversial and contentious subject, intuitively many are hesitant to give credence to the belief a life may be valued economically in any meaningful way. Philosophical and economical criticisms exist both against the whole project of valuing a life (are all aspects of a human life comparable, and reducible to a dollar value?), as well as within the project of valuing a life (is assessing risk taking behaviours the best approach, or are survey studies?). It is nonetheless a necessary concept for policy in the areas of health, insurance and transport, amongst others. It allows for the practical allocation of resources, and investment in cost-effective technologies. It also provides an interesting example of a measure of economic inequities that exist in our world. If we hold morally that all human life has equal value, what are we to think of the tension that exists between this moral position and the differing VSL placed on lives across the globe? What factors are driving this gap, and are they a fruitful area of focus in attempts to improve the wellbeing of the global poor?
Methods of valuing life
In economies, the value of a good or service is in large part determined by the market, supply and demand. There is no such market for human life, and thus alternate methods must be used, which provide highly variable results.
A measure on the value of a human life is an important factor in policy decisions and research. However, a supply-demand economy does not exist for human life, and thus we need to take a more theoretical approach. I will outline a few key methods here, adapted from this high yield summary from Social Value UK. There is no one accepted or unifying method to determining a VSL, but a multitude each with their own advantages and disadvantages.
A crude method – Human Capital
Is a person simply worth what they earn? This is the basis of the human capital approach to measuring VSL. The potential earnings of the individual are approximated based on age, life expectancy and potential future increases in earnings. It is thus sensitive to key demographic factors, and is easy to calculate and compare amongst groups. There are however several limitations to this method. It focuses only on the earnings of the individual, failing to account for life’s intangibles, the value an individual may experience from undertaking leisure activities, personal relationships and general wellbeing. It is also sensitive to income inequalities, valuing the VSL of certain high-earning groups higher than others.
A personal perspective – Contingent Valuation
Individuals are asked what dollar value they would be willing to pay for various levels of improvement to their risk of mortality, or how much they would need to be paid to accept an increased likelihood of death. From this, inference is made to the value placed on one’s own life. This approach goes beyond the ‘low resolution’ Human Capital method to capture the intangible aspects of life, and is thus a more holistic estimate of the VSL. It is however liable to individuals placing unrealistically high values on their own lives, a so-called ‘protest-bid’, which can skew results. Additionally, difficulties with scope insensitivity, the ability to differentiate levels of risk in a meaningful and consistent manner, can result in unreliable individual responses.
Revealed preferences – Consumer Preference Method
Individual choices in a market economy can reveal the monetary value individuals are willing to place on changes to their own safety. If an individual is willing to pay a higher price for a safer product alternative and related reduction in mortality, we can infer the VSL. For instance, what price differential would an individual be willing to pay for a car with, or without, airbags? The main advantage of this method in comparison to the Contingent Valuation method is it relies on revealed rather than stated preferences, thus avoiding issues such as protest-bids. One’s preferences in the market are not solely driven by the difference in risk associated with different product or service choices however. It is therefore important to consider how much safety factors into the individuals purchasing decision.
Differing values for differing populations
Depending on the method and population group being studied, there may be wide variation in the VSL calculated. In all three of the methodological approaches above, a relatively high-income earner in a high-income country will likely have a higher VSL than an individual struggling to find employment in a low-income country. From a purely economic perspective, we can see how the lower valuation of a particular life may lead one to make riskier decisions surrounding health and wellbeing, or give less incentive for governments or private entities to invest in the wellbeing and longevity of the lower-income individual. An excellent example of this disparity comes from a paper by León and Miguel, which looks at the revealed preference VSL between African and non-African travellers making decisions on the transport mode used to travel to the international airport in Freetown, Sierra Leone. travellers had to decide between 4 options, each varying in risk, convenience and cost, namely ferry, hovercraft, water taxi and helicopter. After surveying some 561 travellers on their revealed travel preferences (i.e. the choices they made in the real world), the VSL calculated for African travellers was US$577 000, compared with US$924 000 for non-Africans, an almost doubling of the dollar amount. Further, the sample of African travellers surveyed as part of the study had an average income almost 50-times that of the average African citizen, meaning we should consider this an extremely conservative estimate of the true difference in the VSL between the typical African citizen compared to non-African travellers. The authors show statistically that this difference is driven in large part by differences in income, and the more fatalistic beliefs (the belief that things in the world are determined by fate, rather than believing one has more agency over their future) held by African survey respondents.
What implications does this idea have for our society as a whole? It seems somewhat obvious that those living in low or middle-income countries have significantly less purchasing power in the world economy compared to their high-income neighbours. This revealed valuation provides evidence that individuals may place a lower economic value on their own lives. But is this really the correct way to think about such valuations? Should we perhaps instead adopt a relative measure, something like an individual’s revealed preference VSL divided by the local GDP? If we take this approach, using IMF data and GDP per capita for the African continent for African travellers, and worldwide GDP per capita for all other travellers (no equivalent available data for non-African GDP per capita), we end up with the following calculations:
For African travellers: $577 000/$2 194 = 262.99
For non-African travellers: $924 000/$13 396 = 68.98
This shows African travellers value their life at a level approximately 263 times that of their annual average GDP, compared with non-African travellers who value it some 69 times as much. We do however need to be aware of the selection bias present in the original sample, that the African travellers sampled had incomes that differed significantly from the average found in the population. The quoted rate of the African traveller included in the study was approximately 50 times that of the average GDP per capita. If we apply this 50 times multiplier to our calculation, we get a very different result
For African travellers: ($577 000/50)/$2 194 = 5.26
For non-African travellers: $924 000/$13 396 = 68.98
Not only is the GDP and revealed preference VSL lower for African travellers, the VSL to GDP ratio is also lower. The selection-bias adjusted result suggests the non-African travellers have a VSL/GDP ratio some 13 times higher than African travellers.
The adjusted result suggests the non-African traveller economically values their lives some 13 times higher than African travellers, when corrected for GDP and adjusted for the selection bias present in the original study. Are fatalistic attitude doing the work here to explain the difference beyond the calculated values for GDP and VSL? They perhaps may be contributing somewhat. It may also be argued that the reason for the large difference is that these results reveal an internalisation of the very real differences in what a society is willing to spend to save any one individual’s life. For instance, whilst there may be a certain VSL figure for an individual in a high-income country, it is also true that for instance in Australia, if one were to require an expensive, potentially life-saving but likely futile medical intervention, the economic cost would hold very little weight at the individual level. The main factors being weighed would be the wellbeing of the person and potential for quality-life gained, against the potential pain, harm, or loss of dignity that may result from such an intervention. In such a case, for the individual in this circumstance, the upper bound to the allocation of resources to extend their life is set by what science is able to do to extend or improve a life, rather than economic factors. The same cannot be said in low-income societies. Whilst life-saving interventions that are low-cost, highly-effective and available are theoretically obtainable, an individual’s economic situation or the availability of healthcare services (such as diagnostics, drugs or interventions) provide an upper bound to what can be offered to these individuals. One may point to available universal health care as the factor doing the work in this scenario. If we consider emergency situations however, it is true that a life-saving intervention would be administered to an individual in most high-income societies regardless of insurance or relative financial status. It is possible that individuals living within low-income societies internalise this unspoken valuation that is placed on the willingness to spend to save their lives, and thereby make choices in the real world reflective of the fact that the value they place on their own life is less. This makes for a vicious circle of risky decision making, and makes it all the more difficult to change individual behaviours to look forward to the long-term.
Scale, tractability and neglectedness
Given this information, does it change how we should approach the gap that exist between the equal moral values of all human lives and the VSL across different parts of our global society? The scale of the issue is certainly large, potentially accounting for some fraction of total income inequality across the globe. There may be a significant aspect of neglectedness of focus on both fatalistic attitudes, and the impact of the self-valuation of a life on life quality and quantity. Certainly, it would be of great value to have a better idea of how these factors impact the lives of those living in low income communities around the globe. How tractable the use of this information would be in efforts to combat economic inequalities across the globe and improve the lives of those in poverty is questionable. Changing the perceptions and resultant behaviours of large numbers of people is notoriously difficult, so it is unclear how much impact could be gained from further insights into these specific causal mechanisms would impact the issue at scale.
Conclusion
A lower price on the VSL for individuals in developing nations may go some way to explaining the lack of investment in technologies to improve the lives of those living in these nations. Since individuals are implicitly willing to spend less in relative and absolute terms to preserve their own lives, there is less incentive to develop innovations that will do so. In order to work toward improving the health and wellbeing of those living in low-income societies, there may be value in further research into the utility of relative and absolute VSL estimates as a marker of progress, and tool for gaining a more nuanced insight into the factors underlying economic inequalities.
A 21 year old male presents with ascites and lethargy. He gives a history of fever, jaundice and right upper quadrant pain about one year prior. The walk from his home in an adjacent village took him all of the day yesterday, arriving at the health centre late in the evening. This morning the rapid test available is positive for hepatitis B. The guidelines suggest commencing on lifelong antiviral treatment with tenofovir, entecavir or lamivudine. Our health centre however only stocks tenofovir and lamivudine as part of an all in one medication available for the treatment of HIV. The single drug is available at the district hospital another 30 kilometres down the road, but the patient as a young male does not qualify for government subsidised treatments, he will need to pay. The all-in-one HIV drug however is subsidised, for those with HIV. We perform a rapid HIV test. In the 5-minute window it takes the mixture of blood and solution to migrate down the rapid test strip, I think about the absurdity of the fact that I’m really hoping this guy has HIV.
The aforementioned man is not the first, or the last, who has faced the choice of financial ruin or health. A striking fact of the limitations of resources available in developing settings are the inequalities within inequalities. A patient with malaria, if they’re able to access the health centre in a timely manner, is promptly tested, and treated with effective anti-malarial drugs. Patients with respiratory or urinary tract infections can access antibiotics. Even patients with HIV and TB can access government subsidised treatment regimens. Contingencies aside, in theory treatment is available and free for these conditions. Often these programmes are propped up by government funded programs, local or foreign, or by charities seeking to mitigate poor outcomes from a certain condition.
Previously, I very much would have advocated for the approach to doing good that is purely of QALYs gained or DALYs averted. Whether this be through donating toward insecticide treated bednets, or deworming efforts. However, I’m becoming more convinced of the need to take a more ground up approach to development and health service delivery. It is certainly good to avert a malaria infection or adverse outcome from chronic schistosomiasis, but what is to be said of the dollars spent on the development of a nation wide pharmaceutical infrastructure? How cost effective are these dollars? Is it even possible to quantify or compare these two alternatives?
Top-down, or intervention specific approaches to improving the lives of those in poverty have their advantages. They can be studied, controlled for, and quantified. A program delivering treatment for a specific disease is able to show in an RCT its effectiveness, and thus is well placed to receive financial support in the competitive fight for funding. It is attractive to those aiming to have a meaningful impact in the world, and is recommended as cost effective by charity evaluation bodies. But what of the project of development more broadly? There is certainly at least some value to be gained from contributing to the development of infrastructure and institutions that are able to deliver health care and services holistically to their communities. It is however very difficult to measure, is far more complex and contingent than a ‘narrow’ intervention, and fails to provide an attractive dollar value per life saved.
Additionally, it seems very likely that returns on investments for broad development projects are much less linear than that of their narrow and scalable counterparts. For a Tanzanian project aiming to build a health centre to serve approximately 3000 people quoted approximately $42 million USD, just to build and fit out the centre. This is ignoring ongoing staffing, medication and stock requirements, as well as maintenance, electricity and water. How much good could this money do if given to the Against Malaria Foundation? At an estimate of $3461/life saved, one could hope to save 12 135.221 lives for the cost of this health centre. What should be funded then given the choice? Is the right choice to opt for the bed nets given the more quantifiable certainty of a potential donation to the Against Malaria Foundation? Or is the less-quantifiable chance of contributing to the development of a community a better bet?
The man’s HIV test was negative. We gave him a prescription he could fill at the district hospital, and a referral for a liver ultrasound. I will never know what comes of his journey or treatment. It is extremely important to focus on evidence and outcomes when considering how to do the most good in the field of global health and wellbeing. Evidence back interventions have saved millions of lives, and will continue to do so. The conclusions I have drawn from this experience and from the writings of development economists such as William Easterly who take a stand against interventional approaches to development is that it’s complicated. I don’t think there is perfect solution to how best to spend the next dollar in global health and development, but I do think at least some resources need to be directed beyond RCT backed and dollar-per-QALY driven interventions.